Upper Extremity Fractures
Proximal Humerus Fractures
Definition: Often due to falls or sports injuries.
Special considerations: These fractures can involve the physis (Salter-Harris fractures, described in the general principles tab). They have a high remodeling potential, especially in young children.
Treatment:
Non-operative (sling or Sarmiento brace) for most.
Surgery (e.g., closed reduction with percutaneous pinning) if significantly displaced in older children or adolescents.

Humeral Shaft Fractures
Definition: Fractures of the diaphysis of the humerus that is often caused by falls, high-energy trauma, or birth injuries (e.g., clavicle or humerus fractures during delivery).
Special Considerations: Can cause a radial nerve palsy, which may recover spontaneously
Treatment:
Most heal well with immobilization (hanging arm cast or u-slab splint).
Rarely need surgery unless polytrauma or open fracture.

Supracondylar Fractures
Definition: A break in the humerus (upper arm bone) just above the elbow joint often caused by a fall on an outstretched hand (FOOSH)
Special Considerations
Subtypes:
Extension-type (95% of the time) - Left sided image from below
Flexion-type- right sided image from below
Classification: Extension types are classified by the Gartland classification system as seen in the figure. They include Gartland types I–IV. Flexion type fractures are a rare kind of fracture.
Treatment:
Type I: immobilization
Type II: often closed reduction and casting or pinning
Type III: usually require closed or open reduction and percutaneous pinning (CRPP or ORIF)
Flexion Type: CRPP or ORIF
Complications: Neurovascular injury (anterior interosseous nerve for extension type and ulnar nerve for flexion), compartment syndrome, cubitus varus


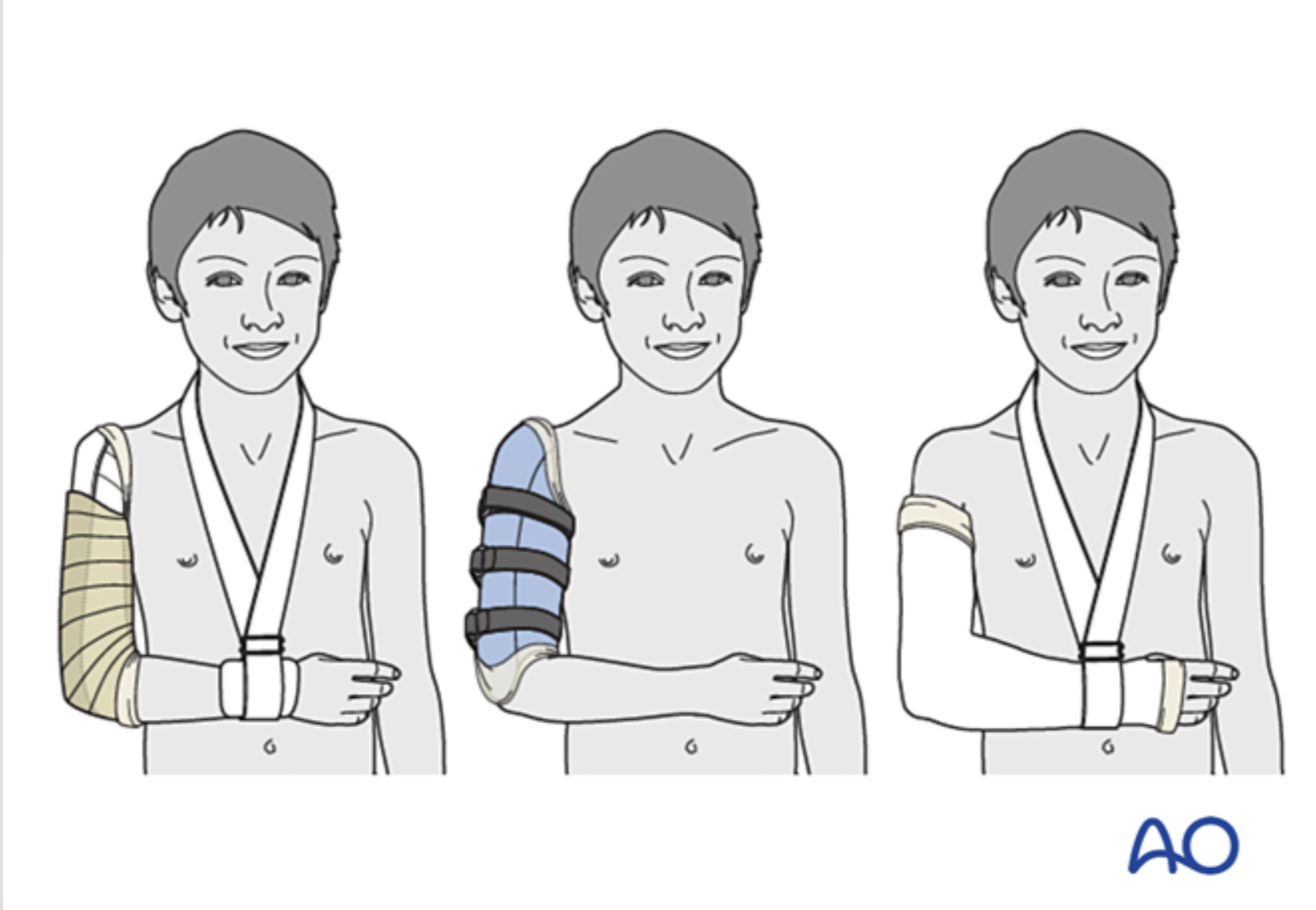
Types of Nonoperative Treatment- Definitions:
From left to right: u-slab splint, hanging arm cast, sarimento Brace
-
Haney S, Scherl S, DiMeglio L, et al. Evaluating Young Children With Fractures for Child Abuse: Clinical Report. Pediatrics. 2025;155(2):e2024070074. doi:10.1542/peds.2024-070074.
Daag Jacobsen S, Marsell R, Wolf O, Hailer YD. Epidemiology of Proximal and Diaphyseal Humeral Fractures in Children: An Observational Study From the Swedish Fracture Register. BMC Musculoskeletal Disorders. 2022;23(1):96. doi:10.1186/s12891-022-05042-0.
Popkin CA, Levine WN, Ahmad CS. Evaluation and Management of Pediatric Proximal Humerus Fractures. J Am Acad Orthop Surg. 2015;23(2):77-86. doi:10.5435/JAAOS-D-14-00033.
Lefèvre Y, Journeau P, Angelliaume A, Bouty A, Dobremez E. Proximal Humerus Fractures in Children and Adolescents. Orthop Traumatol Surg Res. 2014;100(1 Suppl):S149-56. doi:10.1016/j.otsr.2013.06.010.
Abzug JM, Dua K, Kozin SH, Herman MJ. Current Concepts in the Treatment of Lateral Condyle Fractures in Children. J Am Acad Orthop Surg. 2020;28(1):e9-e19. doi:10.5435/JAAOS-D-17-00815.
Hannonen J, Hyvönen H, Korhonen L, Serlo W, Sinikumpu JJ. The Incidence and Treatment Trends of Pediatric Proximal Humerus Fractures. BMC Musculoskelet Disord. 2019;20(1):571. doi:10.1186/s12891-019-2948-7.
Thomson JE, Edobor-Osula OF. Do Pediatric Shoulder Fractures Benefit From Surgery?Curr Opin Pediatr. 2021;33(1):97-104. doi:10.1097/MOP.0000000000000979.
Caviglia H, Garrido CP, Palazzi FF, Meana NV. Pediatric Fractures of the Humerus. Clin Orthop Relat Res. 2005;(432):49-56. doi:10.1097/01.blo.0000156452.91271.fb.
James V, Chng ACC, Ting FLM, Chan YH, Ganapathy S. Lateral Condyle Fracture of the Humerus Among Children Attending a Pediatric Emergency Department: A 10-Year Single-Center Experience. Pediatr Emerg Care. 2021;37(12):e1339-e1344. doi:10.1097/PEC.0000000000002032.
Hohloch L, Eberbach H, Wagner FC, et al. Age- And Severity-Adjusted Treatment of Proximal Humerus Fractures in Children and Adolescents—a Systematical Review and Meta-Analysis. PLoS One. 2017;12(8):e0183157. doi:10.1371/journal.pone.0183157.