Upper Extremity Fractures
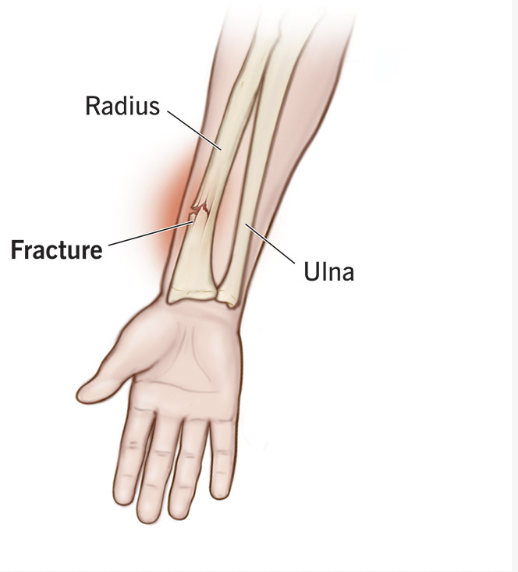
The radius and ulna are bones in the forearm, with the radius in the thumb side and ulna on the pinky side.
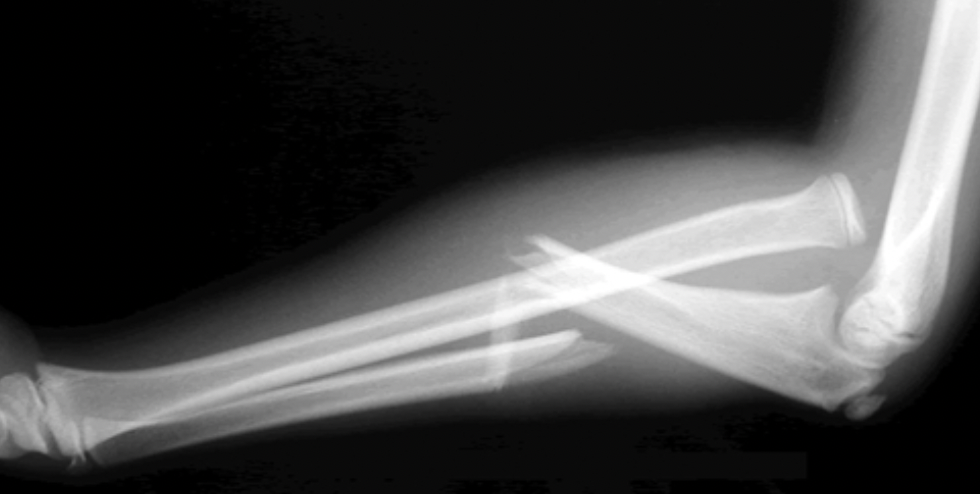
1. Both-Bone Forearm Fracture
Definition: Fracture of radius and ulna and is one of the most common pediatric fractures (40% of all pediatric fractures)
Special Considerations: usually occurs from fall from a height, sporting event, or playground equipment injury (especially monkey bars, trampoline)
Treatment:
Non-displaced: Long arm cast
Displaced: May need closed reduction or surgery (especially in older kids)

2. Greenstick Fracture
Definition: This occurs when one side of the bone breaks but the other side of the bone is simply bent There is no complete break in a greenstick fracture.
Special Considerations: Tend to effect you younger kids (<10 years old) since they have softer and less brittle bones than adults
Treatment: Cast (may need to complete the break to realign)

3. Torus (Buckle) Fracture
Definition: One side of the bone gets compressed and bends without breaking completely through. This is similar to pressing down on an empty paper towel roll that bends on one side but stays intact
Special Considerations: These fractures are very stable
Treatment: Short arm cast or splint for 2–3 weeks

4. Monteggia Fracture
Definition: This occurs when the ulna has a fracture and the radial head has dislocated from the elbow joint
Special Considerations: The annular ligament is usually stretched or ruptures
Treatment: Children can be reduced and immobilized in a cast. If the fracture is open (goes through the skin), unstable, or comminuted, it may require surgery
5. Galeazzi Fracture
Definition: This is when the radius fractures and the ulna is dislocated at the wrist
Special considerations: This fracture is less common in kids, more common in adults
Treatment: These fractures often need surgical management

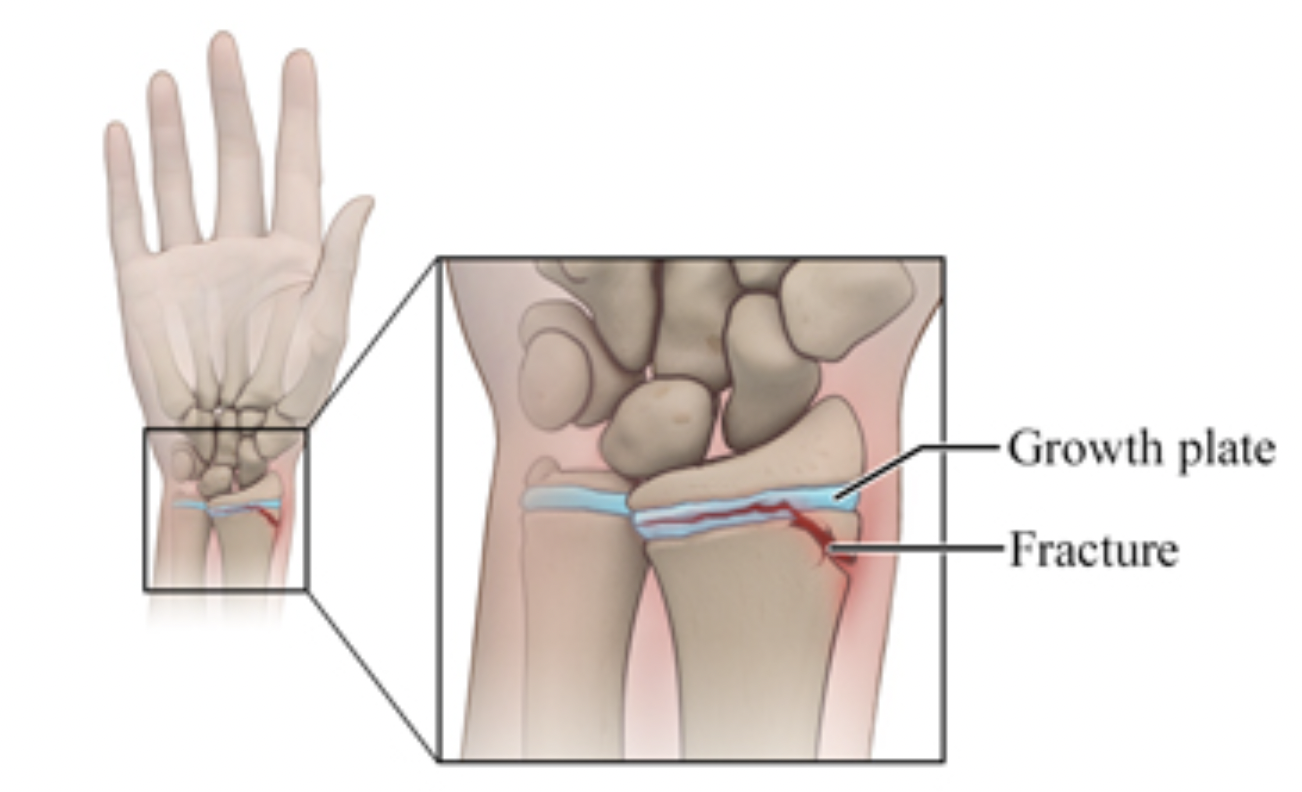
6. Growth Plate Fractures
Definition: This occurs when the growth plate or physis through the wrist is involved in the injury.
Special considerations: Most commonly occur at the wrist. There is a large amount of remodeling potential when fractures occur near or through physis, especially in younger children. But as kids age, growth plate fractures may cause longer-term disfiguration (since there is less room to “grow out” of a deformity”
Treatment: If displaced: gentle manipulation to get the fracture in place and then short arm cast. Try to limit to one attempt to reduce chance of growth arrest (when the physis is damaged and bone is no longer able to grow
-
Rodríguez-Merchán EC. Pediatric Fractures of the Forearm. Clin Orthop Relat Res. 2005;(432):65-72.
Noonan KJ, Price CT. Forearm and Distal Radius Fractures in Children. J Am Acad Orthop Surg. 1998;6(3):146-56. doi:10.5435/00124635-199805000-00002.
Snelling PJ, Jones P, Bade D, et al. Ultrasonography or Radiography for Suspected Pediatric Distal Forearm Fractures. N Engl J Med. 2023;388(22):2049-2057. doi:10.1056/NEJMoa2213883.
Runyon RS, Doyle SM. Splint vs. Cast and Remodeling in Pediatric Forearm Fractures. Curr Opin Pediatr. 2017;29(1):46-54. doi:10.1097/MOP.0000000000000435.
Kubiak R, Aksakal D, Weiss C, et al. Treatment for Displaced Pediatric Diametaphyseal Forearm Fractures. Medicine. 2019;98(28):e16353. doi:10.1097/MD.0000000000016353.
Hansen RT, Borghegn NW, Gundtoft PH, et al. Treatment Preferences in Pediatric Diaphyseal Forearm Fractures: A Register Study. Acta Orthop. 2023;94:32-37. doi:10.2340/17453674.2023.7132.
Stark D, Denzinger M, Ebert L, et al. Therapeutic Approaches to Diametaphyseal Radius Fractures. Arch Orthop Trauma Surg. 2024;144(3):1179-1188. doi:10.1007/s00402-023-05118-z.
Husum HC, Rahbek O, Gundtoft PH, et al. Refracture and Malunion in Pediatric Diaphyseal Forearm Fractures. Acta Orthop. 2025;96:189-194. doi:10.2340/17453674.2025.42851.
Franklin CC, Robinson J, Noonan K, Flynn JM. Management of Pediatric Forearm Fractures. J Pediatr Orthop. 2012;32 Suppl 2:S131-4. doi:10.1097/BPO.0b013e318259543b.
State-of-the-Art Treatment of Forearm Shaft Fractures. (Author and journal details not fully provided in original text.)